Thank you for subscribing to The PA Rx Newsletter!
Today in 10 minutes or less you will learn:
- Do ERs need more staff, security, or both?
- Are brain bleeds contagious?
- Don’t break the bank at the pharmacy!
- Are vital signs that vital?
Do ERs need more staff, security, or both?
 |
If you ever worked in the ER, you know it is chaos. Sometimes there is too much chaos that it becomes unsafe to work. I remember I was 3 weeks into my first job when a patient kicked the attending physician in the back while he was walking away. I thought stuff like that only happened outside of a bar at 2 am!
I have had my fair share of experiencing chaos and mayhem in the ER and in urgent care, we all have. This article sheds light on the escalating crisis of violence against healthcare workers in emergency rooms (ERs), using a scenario involving an aggressive patient as a poignant example. The complex nature of such behavior is explored, considering factors like alcohol, substances, medical issues, mental health disorders, or external stressors.
The distinction between safety and security is emphasized, with safety focusing on protection from harm and security on creating an environment perceived as trustworthy and reliable. Despite advocating for critical safety measures and legislative actions to curb violence, the author questions whether these interventions can fully restore the eroding sense of control and security among ER staff who grapple, not only with physical threats but also with the cognitive demands of a high-stress environment.
The psychological aspect of patient aggression is delved into, highlighting the potential link between such behavior and feelings of powerlessness or a loss of control. The article underscores the importance of a sensitive, yet firm response to restore control, acknowledging that patients acting out may also be victims of systemic challenges. Ultimately, it calls for operational solutions that not only ensure the physical safety of healthcare workers but also safeguard their cognitive and emotional well-being, fostering an environment that promotes the overall well-being of both staff and patients in the ER.
Are brain bleeds contagious?
 |
I know what you’re thinking. This guy is crazy to say that brain bleeds are contagious. Welp. In this study, it was found that recipients of blood from individuals experiencing brain bleeds are three times more likely to suffer brain bleeds themselves. This suggests a potential infectious agent in cerebral amyloid angiopathy.
Some other interesting medical stories from this Medscape article include:
- Red Wine Headaches: Quercetin, an antioxidant in red wine, may cause headaches due to its metabolite inhibiting an enzyme, leading to acetaldehyde accumulation.
- Sexsomnia: A parasomnia causing inappropriate sexual behaviors during non-REM sleep, potentially linked to sleep apnea, deprivation, or certain medications.
- Cleopatra and Beethoven’s Deaths: Studies suggest venomous snakes in ancient Egypt may support the theory of Cleopatra’s suicide. Beethoven’s death was linked to a genetic predisposition, alcohol consumption, and hepatitis B.
- Cold-Water Immersions: Cold water swimming may have physical and mental health benefits, potentially linked to mood-enhancing neurotransmitters.
- Talking About Money vs. Superstitions: Discussing financial constraints could reduce causal illusions, combating superstitions and pseudoscience.
- Impostor Syndrome Among Doctors: Doctors, especially during transitions, commonly experience impostor syndrome, affecting pediatricians and emergency physicians more.
- Unexpected Pathogens: Mycobacterium marinum infection from an iguana bite; discovery of a parasitic worm in the brain linked to ingesting snake eggs.
- Smart Necklaces: SEAL SwimSafe necklace alarms when submerged, preventing drownings. Another necklace detects smoking events and supports smoking cessation interventions.
Read more about it here.
Always remember..
Don’t break the bank at the pharmacy
 |
The U.S. Food and Drug Administration (FDA) has given its approval to Florida’s program that aims to import prescription drugs from Canada, marking a significant policy shift with potential implications for lowering medication costs in the United States. This move is part of a broader effort to address the persistent issue of high drug prices domestically. The FDA’s decision has garnered criticism from pharmaceutical companies, with concerns raised about potential drug shortages and risks to public health associated with importing unapproved medicines.
Florida’s plan involves the initial importation of drugs used in the treatment of HIV, mental illness, and prostate cancer, pending FDA approval for specific medications. However, the pharmaceutical industry, represented by the Pharmaceutical Research and Manufacturers of America, has expressed deep concerns about the FDA’s decision, emphasizing the potential dangers posed by the importation of unapproved medicines from Canada or elsewhere globally. The industry is considering various options to counter this policy shift, asserting that patient access to necessary medicines is critical, but cautioning against compromising public health by importing unregulated drugs. Experts also question the feasibility of significant drug imports, highlighting Canada’s restrictions on drug exports and the FDA’s requirement to protect the public by ensuring a secure supply chain and preventing the introduction of potentially unsafe or ineffective products. Despite these challenges, the FDA’s move aligns with the Biden administration’s broader efforts to address and mitigate the escalating costs of prescription drugs in the country.
Are Vital Signs that Vital?
 |
Short answer: YES.
This breaks me into a story about another busy shift where I’m on roller skates around the clinic trying to discharge patients when my medical scribe tells me there is a patient in room 6 with nasal congestion for one day after a COVID-19 exposure.
I quickly review the patient’s chart, patient medical history, past visits, and vital signs.
PMHx – none
Medications- none
Allergies – none
Vital signs:
HR: 86
O2: 98% on room air
Respirations: 16
BP: 82/50
Temp: 98.6
Obviously the hairs stood up on my neck and my pupils dilated when I saw that blood pressure. I walked in the room of the patient and saw an older male, in no acute distress, wiping his nose. I immediately went to recheck his blood pressure, this time with a better-fitted sphygmomanometer (say that five times fast). Still low.
I asked my scribe to get me the manual BP machine so I could take it myself. I began to question the patient and perform my exam. When I listened to his heart, it was racing a mile a minute and it was all over the place!
I asked the patient if he had any medical problems and when was the last time he went to his regular family doctor.
He confirmed no medical conditions and he went to his doctor 4 months ago with no significant findings.
Manual blood pressure: still low
ECG looked something like this:
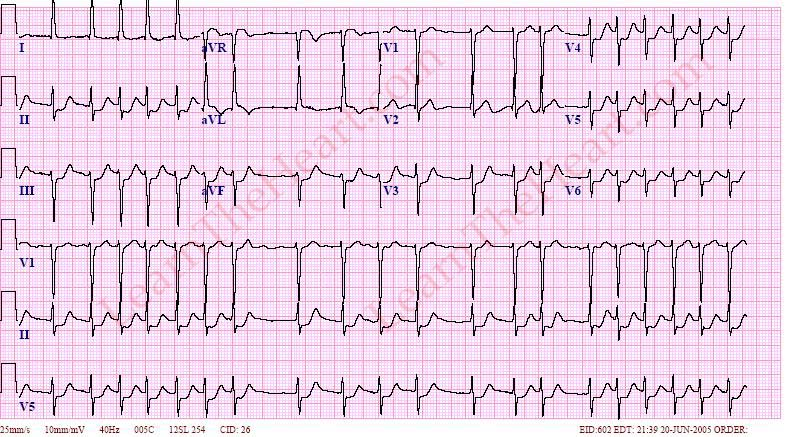 |
My current state of mind when I figured out what was going on:
 |
Next steps were getting the AED to the bedside just in case the patient codes, calling 9-1-1 and starting multiple IVs. Thankfully the patient was transported out of the clinic okay, but those type of patients outside of the ER setting definitely keep me on my toes.
Teaching point:
Are vital signs vital? – Yes. They are called vital signs for a reason. So remember that. (mic drop)
That’s all for today.
For more newsletters and case challenges click here
Preparing for a job interview? Click here for our FREE job interview checklist
Want more question practice? Click here for our affordable 225 question exam with detailed explanations
Thanks for reading,